
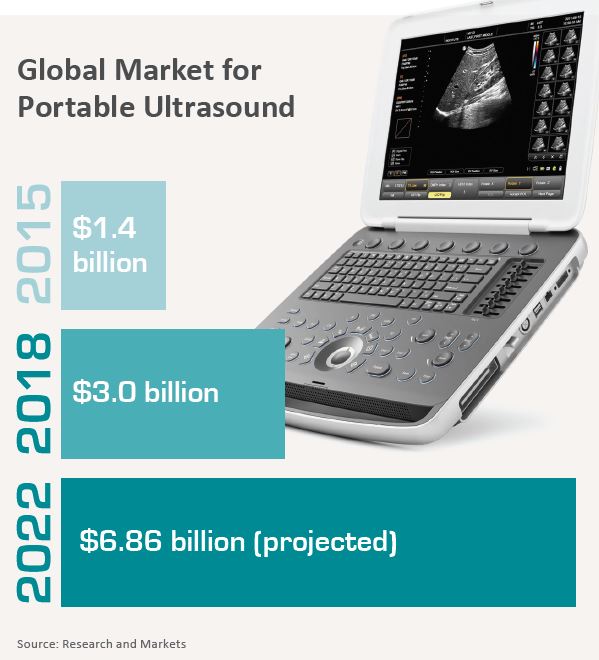
Point-of-care ultrasound has been creating something of a stir over the past few years. The kerfuffle has arisen because POCUS—the acquisition and interpretation of sonograms by nonradiologists—is now routinely used not only in emergency rooms but also in ambulances, at accident sites and wherever else a patient in need might happen to be located.
Some radiologists have expressed apprehension about this trend. Their primary concern is ensuring authoritative reads in the ER and beyond.
For their part, emergency physicians increasingly embrace POCUS with unmistakable enthusiasm. They tend to appreciate its clinical capabilities too much to be slowed on the job by turf issues.
At least, that’s the perception. To uncover the reality, RBJ asked for input from physicians in both camps.
Rad’s Eye View
Contrary to what some emergency physicians may believe, radiologists surely do recognize the value of POCUS in the emergency department in certain situations, such as when patients are too ill to undergo an ultrasound study in a hospital radiology department.
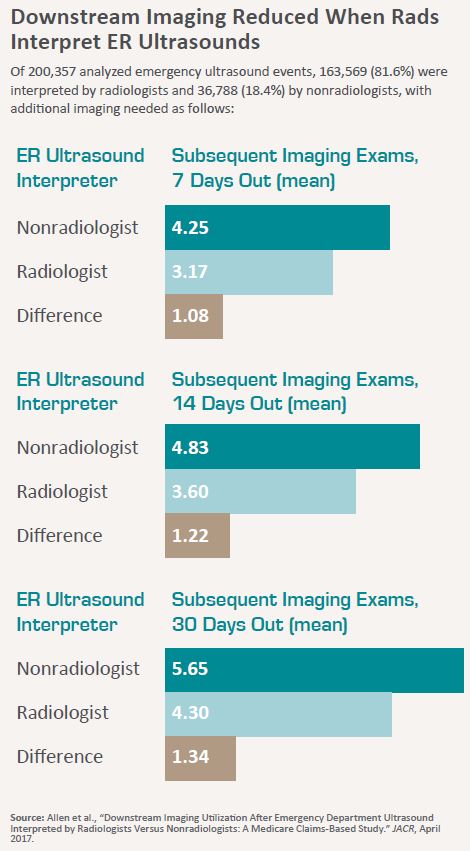
“Ultrasound in the emergency room has, for example, eliminated the need for peritoneal lavage in critical trauma patients,” says Alabama radiologist Bibb Allen Jr., MD, a past president of the American College of Radiology. Allen was the lead author of “Downstream Imaging Utilization After Emergency Department Ultrasound Interpreted by Radiologists Versus Nonradiologists: A Medicare Claims-Based Study,” published in the April 2017 issue of JACR.
Conducted using 5% Medicare Research Identifiable Files from 2009 through 2014, the study found that the rate of downstream imaging after an initial POCUS in the emergency room is significantly reduced when the sonogram is interpreted by a radiologist rather than a nonradiologist.
Just as significantly, Allen explains, there is no denying that younger emergency medicine practitioners have had a significant amount of ultrasound training to which established physicians have not been exposed.
“However, we as radiologists have a lot of certifications, and we challenge others to conduct POCUS at the same level of care that we can,” Allen says. “This is not to say POCUS shouldn’t be done in the emergency department, but it needs to be done at the same level of care and competence patients would receive from a radiologist. And as it stands now, that isn’t always possible.”
Andrew Rosenkrantz, MD, of NYU Langone Medical Center, a co-author of the JACR study, amplifies the point.
“We’re not saying interpretations cannot be done by nonradiologists or should not be done by nonradiologists,” Rosenkrantz says. As long as there is close collaboration and teamwork, regardless of imaging modality, he adds, nonradiologists surely deserve a place at the imaging-interpretation table.
The Take in the ER
A voice from across the proverbial table agrees on the value of communication and collaboration between radiology and emergency med.
“An emergency physician who performs POCUS might start out with a focused question, such as whether or not the patient has gallstones,” says Michael Zwank, MD, of the emergency department at 454-bed Regions Hospital in St. Paul, Minn. “With experience, the provider might start asking about common bile duct dilation. A radiologist, however, may be concerned as to whether this may naturally progress to other questions, such as about the existence of liver lesions or pancreatic lesions, or if more advanced assessments [would be appropriate].”
Zwank’s take on the matter is informed by his daily work at Regions, where he directs an emergency ultrasound fellowship and co-chairs the hospital’s POCUS committee. He also teaches emergency medicine at the University of Minnesota. And on his hospital webpage, he speaks directly to patients about POCUS.
“One main focus of my practice and teaching is on bedside ultrasound,” he writes. “We are using ultrasound more and more frequently to help diagnose and guide patient care. We use it for everything from looking at the function of a patient’s heart to locating the toothpick or glass that is stuck somewhere in a patient’s foot.”
A Question of Clinical Intent
Zwank emphasizes that, above all else, he would like radiologists to understand why POCUS studies have “different intent” and goals than ultrasound exams performed in the radiology suite. He deems the aim of POCUS to answer focused questions rather than to provide comprehensive studies, adding that answering such questions paves the way for expedited and improved patient care.
“POCUS can at times replace radiology-performed ultrasound, but just as often, it can complement it,” Zwank tells RBJ. For instance, he says, finding hydronephrosis with POCUS in an appropriate patient can help to confirm a diagnosis of renal colic and expedite discharge. Similarly, detecting no gallstones with POCUS would likely lead a physician to order a CT scan to evaluate for kidney stones or appendicitis in a patient who presents with nondescript pain in the right side of the abdomen or back.
Zwank wants to see more radiologists acknowledge POCUS’s usefulness in cases where a patient is critically ill and minutes really matter. This, he says, is the locus of the modality’s greatest value.
He cites the example of a young woman brought to the ER following a resuscitated cardiac arrest. The patient was complaining of severe shortness of breath and was hypoxic, tachypneic, tachycardic and hypotensive, Zwank recalls. While most physicians would have focused on identifying a massive pulmonary embolism as the cause of the patient’s symptoms, POCUS showed good cardiac function and free fluid in the abdomen. A subsequent CT of the abdomen revealed the presence of a large liver laceration. The culprit: overaggressive CPR.
This, Zwank notes, “is an example of where POCUS played a critical role in the management” of a particular patient.
Patients First
Emergency-med specialist Rachel Liu, BAO, MBBCh, of Yale New Haven Health seconds Zwank’s points and adds that, ideally, radiologists will accept that the “end game” of POCUS is the same for all physicians.

“Both emergency physicians and radiologists are first interested in providing the best possible care to patients,” states Liu, who directs Yale Medical School’s POCUS education program.
“For emergency physicians, the main benefit of POCUS is saving time while pursuing correct treatment pathways, particularly when there is extremely high diagnostic uncertainty coupled with high morbidity or mortality associated with certain diseases,” Liu says.
Applications that help achieve these aims, Liu continues, are essential tools for emergency physicians because they facilitate consistency of care through shift changes without slowing patient throughput.
That’s adding a lot of value in a time when many ERs across the country are beleaguered by overflowing waiting rooms on top of admitted patients boarding in the ER till an inpatient room is ready.
Liu says emergency physicians understand radiologists’ concern about the importance of education for those who perform POCUS on patients in emergency room settings. “We get it,” she tells RBJ. She points out that emergency ultrasound training directors are indeed serious about providing robust instruction for residents, fellows and colleagues who didn’t have a chance to learn POCUS during their residency.
Trainers also are dedicated to upholding responsible practices when using POCUS, Liu adds. This includes making sure trainees understand the modality’s limitations and know how to document findings with required image archiving—“which mirrors the same setup used by radiologists.”
 Some radiologists, Liu says, may not be aware that the emergency medicine specialty has developed rigorous, standardized QA programs across hospital systems. Guidelines and policies regarding safe, effective POCUS have been written by national organizations in partnership with the American Institute of Ultrasound in Medicine (AIUM), she explains. Additionally, in 2018, the American Board of Medical Specialties (ABMS) approved a focused practice designation in advanced emergency medicine ultrasonography. Going forward, this will involve a written exam and will be open to ultrasound fellowship-trained emergency medicine candidates.
Some radiologists, Liu says, may not be aware that the emergency medicine specialty has developed rigorous, standardized QA programs across hospital systems. Guidelines and policies regarding safe, effective POCUS have been written by national organizations in partnership with the American Institute of Ultrasound in Medicine (AIUM), she explains. Additionally, in 2018, the American Board of Medical Specialties (ABMS) approved a focused practice designation in advanced emergency medicine ultrasonography. Going forward, this will involve a written exam and will be open to ultrasound fellowship-trained emergency medicine candidates.
Looking for ‘Logistical Flexibility’
Both Liu and Zwank foresee radiologists playing a key role in the POCUS space, and that goes for clinical as well as educational zones. However, they believe, optimizing the collaboration will require more meetings of the minds to hash out clinical particulars and a willingness to adjust educational cultures.
Further, they suggest, radiologists would do much to advance the collaboration by showing an openness to re-train in skills not typically reinforced in radiology, such as physical examination.
Liu mentions another attribute that would help smooth the road ahead: “logistical flexibility.” Asked to expound, she says radiology professors who teach in workshop settings or hospital rounds can quickly find a colleague to cover during these hours, even when the request is made on short notice.
“With us, this isn’t possible,” Liu says. “We have to attend or teach workshops on our days off. That logistical difference complicates the whole workshop issue.”
Calling All Collaborators
According to Allen, POCUS can best be optimized when emergency medicine physicians and radiologists cooperate to prioritize quality assurance. For example, he suggests, emergency-med physicians should ensure that POCUS exams are properly documented and archived so that follow-ups on initial studies are easier to conduct. At the same time, radiologists should support emergency med with these follow-ups.
Allen adds that the advent of clinical decision support solutions for POCUS should push the collaboration and QA envelope further. The ACR is currently teaming up with several emergency medicine societies to develop these tools, he notes.
Rosenkranz expresses a similar perspective about the need to jointly focus on imaging quality.
“There should be less worry about whose territory is whose and more working together on supporting each other,” he says, adding that one major gain to be had from the change of mindset is “less need for unnecessary downstream imaging.”
Zwank says he and his colleagues at Regions Hospital have been “very fortunate” to have a collaborative partnership with their radiology department colleagues.
At the same time, he acknowledges that achieving a high degree of interdepartmental cooperation on POCUS remains difficult in many institutions.
“Many of the hardest challenges stem from the initial ‘turf battle’ that naturally occurred when POCUS was first evolving,” Zwank observes. “More recently, I think this happens because of a lack of understanding between the two
departments.” It bears repeating, he says, that “there are big differences between ultrasound exams performed in the radiology department and those performed in the emergency department. If we understand these differences, better relationships will follow.”
Moreover, Zwank notes, those POCUS studies that are frequently brought to radiologists’ attention are ‘misses’—and when radiologists see one, it’s natural for them to question the competency of the provider who performed the study and interpreted the images.
“The best way to assure competency is the same as with any aspect of medicine,” he says. “You need an effective quality assurance program in place to review POCUSes.”
Good Habits Are Gettable
Open minds on both sides of the table, along with open dialogue among all constituents, will advance the cause of collaboration and cooperation, Zwank says.
Liu sees the value in “continuing dialogue across both specialties to understand viewpoints and clinical usage regarding POCUS applications,” which she perceives as having the potential to increase cohesion. Expediency can be promoted, and costs reduced, by forming research partnerships across multiple specialties and developing algorithms that involve combining POCUS with other imaging modalities.
She’d also like to see collaborative research exploring clinical as well as cost outcomes related to algorithmic approaches.
“This is all clinical, but habits regarding placing orders and knowledge about diagnostic modalities themselves form during medical school and residency,” Liu says. “Partnerships in education or co-teaching to improve understanding
of the benefits and limitations of each diagnostic modality, along with co-teaching of POCUS workshops or case conferences that incorporate clinical decision-making in both radiology and emergency medicine didactics, may help.”
Stethoscope with Soundwaves
Conceding that the examination of data conducted for the Medicare claims-based study was limited because those data were aggregated and came from a single source, Allen says POCUS could potentially assume a significant diagnostic role in the emergency department.
However, he does not envision this coming to fruition until a study at the examination level helps to create a greater understanding of the disparity between radiologist and nonradiologist use of downstream imaging following interpretation—and until concrete means of ensuring consistency of image quality are implemented.
“In certain ways, POCUS has become the modern-day stethoscope for kids on ambulance duty,” Allen says. “For instance, someone can put a Doppler on a patient on the way to the hospital if they’re worried about an occlusive [condition]. But that’s not a complete ultrasound.”
Be that as it may, POCUS is growing within emergency medicine. Its expansion is especially noticeable in internal medicine subspecialties, intensive care and family practice, sources say.
Meanwhile POCUS is so user-friendly that middle schoolers can perform scans of acceptable clinical quality and then pass along their skills to classmates. A study at UC-Irvine, published last February in the World Journal of Emergency Medicine, showed as much. John Fox, MD, and Shadi Lahham, MD, together with a 13-year-old student, launched their novel study (“Can an 8th Grade Student Learn Point of Care Ultrasound?”) after noting that POCUS is increasingly conducted by nonprofessionals in underdeveloped areas of the world.
As the Technology Turns
Across the country at Yale New Haven, Liu anticipates that the increasing popularity of relatively inexpensive pocket devices—and a new policy on their appropriate use developed by the American College of Emergency Physicians—will increase healthcare’s appetite for POCUS, particularly at community and clinic-based practices.
“Specialty organizations are, and will be, working to define their interests and scopes of practice, which will likely continue to expand as more applications become clinically relevant,” Liu says. “More medical graduates will come into residency with some cursory knowledge and technical know-how regarding POCUS practices. And applications now considered to be relatively novel—like high-frequency ultrasound and contrast-enhanced ultrasound—may become more mainstream as utility within the emergency and outpatient settings is proven.”
Which is to say that POCUS is a work in progress on more fronts—and in more departments—than one. Keep an eye on the moving transducer.