
Opto-acoustic Imaging: A new modality changing the future of breast imaging

When it comes to breast imaging, a few new technologies have improved the visualization of lesions and diagnostic procedures. But a new modality could change the game completely.
The new modality, opto-acoustic/ultrasound (OA/US) or photoacoustic (PAI) imaging, is indeed a game-changer. And here’s what you need to know about it, how experts see it improving the breast cancer diagnosis process, and how it’s projected to reduce the need for extra diagnostic imaging exams and breast biopsies by a lot.
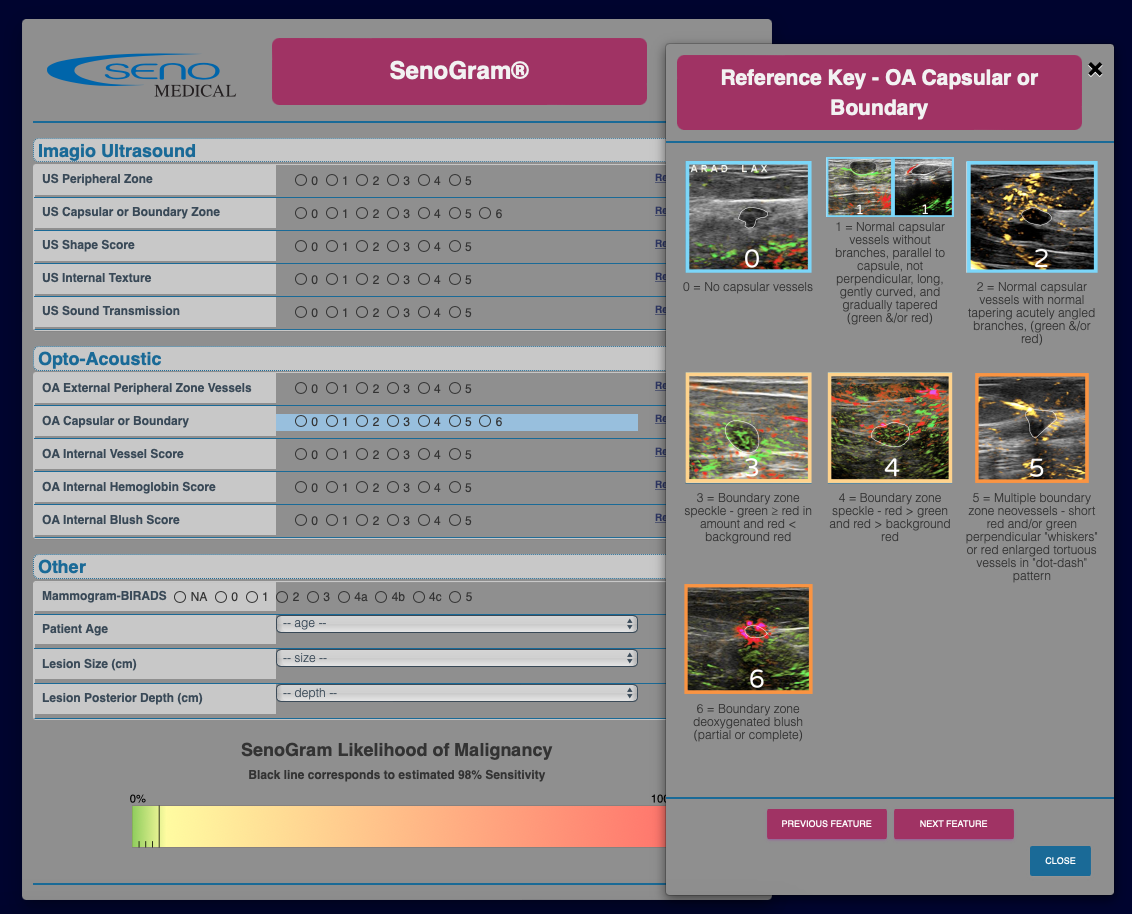
This newest, hybrid imaging modality uses laser light to add perfusion and oxygenation information to conventional ultrasound technology in real time. The high-resolution morphologic ultrasound images are merged with an opto-acoustic functional color-map, so radiologists can see anatomy and function at the same time.
This fused anatomic and functional information looks to transform the breast cancer diagnostic journey both clinically and economically. Since the modality includes ultrasound, it can replace an ultrasound unit in the diagnostic pathway. Potentially, OA/US could be positioned after screening mammography, enabling more confidence in assessing whether or not to recommend biopsy of masses.
Experts see OA/US improving the breast cancer diagnosis process by reducing both duplicative diagnostic imaging exams and breast biopsies of benign masses, saving an estimated $4.9 billion annually for the healthcare system. Early studies even indicate that OA/US can help physicians better assess the type of breast cancer, which may predict its response to treatment over time.
“This is equivalent to the step between 2D and tomography,” notes Kenneth Kist, MD, a radiologist who recently retired from UT Health San Antonio who was part of the PIONEER multicenter clinical trial as well as a next-generation clinical study using OA/US technology. “It has a lot of additional information.”
How Opto-acoustic/Ultrasound Works
Seno Medical’s Imagio® Breast Imaging System, which is now FDA-approved and available for sale in the U.S., includes software and hardware that produces opto-acoustic (OA) images along with high-quality ultrasound images of the breast. A sonographer or radiologist uses ultrasound first to assess any focal areas of clinical or imaging concerns for the presence of a mass. If a mass is found, OA/US can then be turned on to reveal the functional and anatomic features of the breast mass. OA/US does this by pulsing a light beam into the breast to demonstrate the presence and type of blood vessels and the relative degree to which oxygen is present in the blood vessels that lie within the breast mass and its surrounding tissues.
An AI “digital assistant” clinical support tool, the SenoGram®, helps breast imagers to efficiently and confidently assign a Likelihood of Malignancy (LOM), a BI-RADS category, and to make recommendations about the need for biopsy from the OA features that they see. The OA technology allows for the physician to differentiate malignant masses as small as 3mm from benign masses. For breast masses that are initially assigned BI-RAD scores of 3-5 using US alone, OA/US allows for improved classification compared to ultrasound alone. OA mode is not indicated for ultrasound BI-RADS 1 and 2 findings.

“This is game-changing for breast cancer imaging in that we get functional information—that we would normally get from advanced imaging—but with ultrasound”
- Basak Dogan, MD, Director of Research at UT Southwestern Medical Center’s Harold C. Simmons Comprehensive Cancer Center
“This is game-changing for breast cancer imaging in that we get functional information—that we would normally get from advanced imaging—but with ultrasound,” says Basak Dogan, MD, director of research at UT Southwestern Medical Center’s Harold C. Simmons Comprehensive Cancer Center.
“This makes you a better radiologist, having more and deeper information,” notes Jeroen Veltman, MD, PhD, a breast radiologist within MRON (Radiologie Oost-Nederland) who is also responsible for breast and prostate imaging in the ZGT Hospital in Hengelo in the Netherlands. As chair of the breast imaging section of the Dutch Radiology Society and an assistant professor within the Multi-Modality Medical Imaging (M3I) group at the Technical University of Enschede, Veltman says, “We can decide more certainly with this anatomic and functional information what is the right path for the patient.”
Limiting unnecessary biopsies when using OA/US breast imaging
Currently, more than 10% of all women who undergo a diagnostic mammogram will go on to have a breast biopsy. In 71% of cases, the biopsied mass proves to be benign. The patient stress, weeks of waiting for results, discomfort, hassle, and expense were unneeded.
That’s what opto-acoustic ultrasound is seeking to change.
“The primary benefit of this technology is that it can help the patients avoid the biopsy ordeal. [With OA/US], we’re finding that we can more correctly categorize masses we would normally biopsy based on ultrasound features alone,” says Dogan. “In the latest reader study, we found that about 15% of biopsies would have been avoided, and that's without losing significant sensitivity.”
By more accurately choosing which women truly need a biopsy, Seno Medical estimates show the U.S. healthcare system could save some $3 billion in biopsy costs alone, decreasing the $4.3 billion currently spent annually on biopsies to about $1.3 billion. They also predict a reduction in the number of false positives by 75% based on their more recent real-world studies.
And add to that a 46% reduction in first diagnostic imaging exams and a 60% reduction in unneeded second or third imaging exams (because OA/US is the stopgap in providing the needed information to send or not send a patient for biopsy) and just by making OA/US part of the care path, the total estimated savings to U.S. healthcare could amount to $4.9 billion.
Based on interim data from the CONFIDENCE Registry Study for Imagio® Breast Imaging System—a prospective, controlled multi-center observational registry that plans to include 12 sites and seeks to enroll 600 patients by 2024, Seno estimates that implementation of OA/US could result in a 75% reduction in unnecessary biopsies.
“This can help us save on costs for both the patients and the payers, and we have to think about that,” Kist says. “Both the insurers and the federal government are on the hook for a lot of money, and that's a big deal in current times. So, it would be nice to see us more rationally use evidence to decrease the number of biopsies that are unnecessary, and to feel more confident going forward with the procedures that are needed.”
While no physicians want to recommend unnecessary biopsies, until now they lacked the tools needed to confidently make the decision not to recommend biopsy. Before OA/US, in a large percentage of benign masses following a worrisome or palpable mass, even when doctors felt that the likelihood of cancer was relatively low with ultrasound alone, they could not predict the likelihood of malignancy low enough to avoid recommending biopsy. Now OA/US dramatically improves their ability to predict that a benign mass is, indeed, benign, and enables them to more confidently avoid having the discussion to biopsy.
Veltman explains the common conundrum with an example: “Do I actually want to perform a biopsy on a probable fibroadenoma in a 34-year-old? The chance that I'm wrong [about being benign] is very low, but the protocol says I have to do a biopsy.”
That’s where OA/US comes in and can change the calculus, says Veltman, who was part of the MAESTRO study as well as the CONFIDENCE real-world clinical study. “Any patient with a detected lesion on ultrasound can benefit from photoacoustics because we need to type the lesion. We need to be sure of the right course for the patient, probability of malignant or benign, to biopsy or not. This can provide better care for patients and save costs, too.
Thanh Van, MD, director of Breast Imaging and Intervention at UT Health San Antonio who also participated in the next-generation clinical study using Imagio®, considers OA/US imaging especially helpful in women whose mass falls into the BI-RADS 3, or “probably benign,” category, that can be potentially downgraded to BI-RADS 2.
“Additionally, for the BI-RADS 3 women who are really anxious about it, it could give a measure of assurance that you can follow it [instead of taking a biopsy],” she says.
A second opinion before skipping a breast biopsy

"This makes you a better radiologist, having more and deeper information. We can decide more certainly with this anatomic and functional information what is the right path for the patient.”
- Jeroen Veltman, MD, PhD, Breast Radiologist within MRON
Although the most obvious use case for OA/US is downgrading risk, Veltman also notes that in some circumstances it can be helpful to add extra scrutiny in cases where physicians may otherwise be tempted to skip a biopsy.
“We often talk about downgrading, but I think OA/US can be very helpful in upgrading when necessary,” he says. “With the press of a button, you can put it on—and if it is a very active legion, you don't even think about not taking the biopsy.”
That can be especially helpful in instances where a patient doesn’t fit the usual profile of a person with breast cancer, either due to age or other health circumstances, and it may be natural for doctors to downplay their risk. In these instances, OA/US can act as a second opinion and a neutral check on that emotion.
“Doing an ultrasound and finding a lesion in the breast can bring a lot of psychology with it,” he says. “For example, if you have a young patient, you don't want to believe that it’s cancer. But if you put on photoacoustics and it's very active, you know you have to biopsy. It can prevent you from thinking too lightly of a lesion.”
The physicians agree Imagio® can simply be used as a kind of second opinion in cases where doctors may be on the fence.
“It goes both ways,” Van says. “If you think it’s benign and the OA/US doesn’t show any suspicious features, you’re like, ‘Oh, good. That just confirms it. I can safely follow without a biopsy.’ Or if you look at it and there are suspicious features such as vascularity or increased metabolism, you can say, ‘Well, I’m going to biopsy the lesion.’”
Predicting the course of cancerous breast lesions, and the type of cancer
In addition to helping doctors determine whether a lesion is cancerous, Dogan notes that her research shows OA/US also can reveal key prognostic information about the potential course of cancerous lesions over time as well as the type of cancer, such as triple-negative or HER-2 positive.
“The [Imagio®] unit shows oxygenated and deoxygenated blood, as well as the concentration of blood, and those [features] have been shown to be predictors of how the breast cancer is going to behave,” she says. “How aggressive is it going to be? Is it going to metastasize?”
The real-time images from OA/US also can help radiologists predict lymph node metastasis just by looking at the cancer, since the images can reveal hypoxia—a deficiency of oxygen—in the tumor, which Dogan notes drives metastasis.
“We presented a study in which we found that it [OA features] correlates with lymph node metastasis in breast cancer. Cancers with no metastasis showed significantly different features compared to those with metastatic nodes,” she says. “This was just based on imaging the primary cancer without the need to image the lymph nodes.”
If radiologists spot hypoxia on OA/US, it can prompt them to image or biopsy the axilla, and in general take a more rigorous approach to considering axillary lymph node metastasis.
OA/US also can help to determine whether breast cancer is triple-negative or HER-2 positive, Dogan notes.
“Our findings, published in Radiology, showed that certain molecular breast cancer subtypes show distinctive optoacoustic features. Hormone-receptor-expressing cancers show more extrinsic vascularity and hypoxia pattern of optoacoustic features, compared to triple-negative and HER-2 positive types of cancers which show higher intrinsic optoacoustic feature scores,” she says.
This information can be vital to helping doctors determine the best course of treatment for each individual patient. Also, unlike a biopsy, which relies on a small sample that may not be representative of the entire lesion, OA/US offers a more comprehensive and complete outlook.
“Cancers are frequently heterogeneous,” Dogan says. “Oncologists treat patients based on small biopsy samples. But sometimes those are not really representative of the whole entirety of tumors. We wonder, ‘Does the patient actually have a different type of cancer, and we just didn’t capture the receptor status because we biopsied one part of the tumor and the receptor expression was elsewhere?’ It's so groundbreaking to be able to get that information just off of handheld ultrasound.”
Assessing the success of treatment for a specific patient using OA/US
When breast cancer therapy is underway, OA/US may be able to play a key role in helping patients and their doctors determine whether the treatment is effective, even at a very early stage.
This phenomenon is something Dogan is actively studying as part of the feasibility neoadjuvant study, which she led, and she notes that her early findings are promising.
"We're scanning the patients as early as a single cycle after their chemotherapy and finding, interestingly, very dramatic changes that we weren't even aware of, because [prior to the study] we weren't really scanning the patients at that time point,” she says. “We find that the tumor doesn't start shrinking until much later, but I'm observing that the optoacoustic features are showing changes much earlier.”
Dogan says she has even noticed more dramatic early changes in triple-negative patients who are receiving immunotherapy, which she hopes to explore more in-depth as the study continues.
“The patient is really looking for an indication that shows, is this treatment working?,” she says. “And they want to know the answer before they receive months of toxic and expensive treatment.”
“Especially in large markets and large cities, where hospital systems compete against each other, it's nice to be able to say that our radiology practice offers the newest technology, including cutting-edge opto-acoustic imaging. When it comes to healthcare, women seek out technologies that can help them. This could be one.”
- Kenneth Kist, MD, Retired Radiologist at UT Health San Antonio
The right choice in breast imaging for discerning patients
Patient awareness is growing too, with women offering interviews on the success of this new imaging modality. “A patient of mine did an interview with NBC5,” Dogan says. “She kept telling me, ‘Doctor, people need to know about this and why it is so great for patients.’
Like the early days of breast tomosynthesis when women started seeking out centers offering the exam, Kist sees OA/US becoming a differentiator for breast imaging centers, departments and groups.
“Especially in large markets and large cities, where hospital systems compete against each other, it's nice to be able to say that our radiology practice offers the newest technology, including cutting-edge opto-acoustic imaging,” he says. “When it comes to healthcare, women seek out technologies that can help them. This could be one.”
Van agrees: “I think it would give women an extra level of confidence. I think women are just more aware and they seek out technology. This will be one they learn about and find facilities that offer it.”
Opto-acoustic may be the imaging technology of the future
With OA/US offering benefits that mammography, tomosynthesis, breast MRI or PET/CT simply do not—for both patients and physicians—it’s easy to see how the new modality could quickly take off, starting with replacing standard ultrasound machines at larger hospitals and specialty breast centers, and trickling down to more practices as the technology gains confidence among physicians.

“It can be hard for patients to tolerate breast MRI scan,” as Dogan notes. “Many reject it because there’s contrast and they have fear of closed spaces. Others have rods or metal in their bodies that are impediments to scanning them successfully. It can be good, but frankly our knowledge of MRI has come to a plateau. The majority of what it shows is anatomy. The good thing about Imagio® is it is much easier for the patient to tolerate; there’s no contrast but it provides intrinsic tissue contrast of oxygenated and deoxygenated blood.”
And as Kist adds: “At this point, people who are experienced with breast imaging may say, ‘Oh, I don’t think I really need this extra information.’ I think we’re deceiving ourselves on that. I think that’s hubris.”
Van calls Imagio’s® ultrasound quality impressive, noting that she has already requested an Imagio® OA/US for the new mammogram center that UT Health is in process of establishing. “The ultrasound itself is among the best I have seen,” she says. “The detail it offers is beautiful.”

“The training was excellent, getting us comfortable with a new way of scanning. Once you scan a few patients, say five or six, you get the feel of the system and gain confidence in what you are seeing in the images.”
- Thanh Van, MD, Director of Breast Imaging and Intervention at UT Health San Antonio
Dogan notes that she can see small vessels she could not discern with MRI or Doppler.
The learning curve is easy and training comprehensive, the physicians agree, as they each say they began to feel comfortable with the system after just a handful of scans.
“Of course, there’s a learning curve,” Van says, “like with anything new, to use the grayscale then the opto-acoustic transducer. But the training was excellent, getting us comfortable with a new way of scanning. Once you scan a few patients, say five or six, you get the feel of the system and gain confidence in what you are seeing in the images.”
“You get used to the imaging and shift towards recognizing certain patterns, and you gain confidence in what you see and the biopsy outcomes,” Dogan says. “Radiologists are starting to recognize this technology and learn it. It's worthwhile.”
And as Veltman adds, “Interpretation we need to learn, but using the SenoGram makes it remarkably easy. It makes you better, correlating acoustics and ultrasound. Scanning is easy and quite robust. I was surprised at how good you get quickly.”
As physicians realize the potential of the new OA/US modality for imaging and decision pathways for patients and physicians—from improving diagnosis to typing cancers to predicting outcomes to analyzing treatment effectiveness—we’ll all be watching as facilities adopt OA/US (PAI) and see how it earns its place in the care pathway.
“Just like contrast enhancement is different than the black and white anatomy that we saw initially,” Kist says. “Just like Doppler was different, and added additional information and honed our diagnostic and predictive models. This is a really valuable addition. This technology will be a significant player.”