
AI model nearly halves false positive rates for lung cancer CT screenings
An artificial intelligence tool designed to assess lung nodules can effectively detect cancer while also reducing false positives, according to new research.
The study, published Tuesday in Radiology, analyzed data from multiple international lung cancer screening trials. Conducted by researchers at Radboud University Medical Center in the Netherlands, the findings highlight how AI could improve the accuracy of lung cancer screening, which is known to be hindered by high false-positive rates. Reducing these figures could lower unnecessary procedures and the associated costs while also easing patient anxiety concerning CT results.
“Deep learning offers promising solutions, but robust validation is essential,” lead researcher Noa Antonissen, MD, a PhD candidate at Radboud, said in an RSNA news release on the findings. “AI accounts for factors that we might not even see on the CT scan to further assess a nodule as likely to be malignant.”
Researchers trained their algorithm on more than 16,000 nodules from the National Lung Screening Trial. Its performance was then validated using CT data from three other European trials. Combined, the algorithm was tested on data from over 4,000 participants, most of whom were older male smokers, with nearly 8,000 nodules.
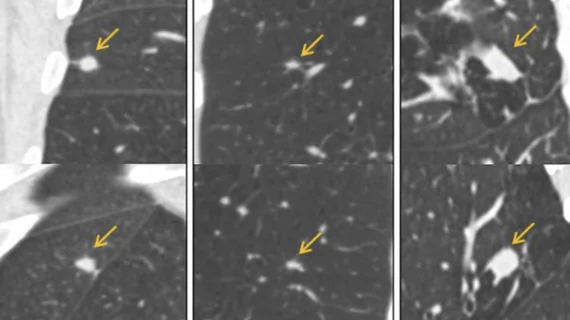
AI’s performance was compared to that of the widely used PanCan model, which estimates cancer risk based on patient information and nodule characteristics. The algorithm consistently matched or outperformed the PanCan model, especially for intermediate nodules between 5 and 15 millimeters, which are often subject to diagnostic uncertainty. In these nodules, the AI’s accuracy achieved an AUC as high as 0.95; in comparison, PanCan yielded an AUC of 0.91. Furthermore, the AI reduced false positives by nearly 40% when compared to the conventional model.
“We selected nodules sized 5mm–15 mm, due to their diagnostic challenges and frequent need for short-term follow-up,” Antonissen said. “Accurate risk classification of these nodules could reduce unnecessary procedures.”
Though the team is encouraged by their findings, they caution that additional prospective clinical validation is needed before the algorithm can be implemented into lung cancer screening workflows.

In addition to her background in journalism, Hannah also has patient-facing experience in clinical settings, having spent more than 12 years working as a registered rad tech. She began covering the medical imaging industry for Innovate Healthcare in 2021.