
MSSP Is Changing. Should Radiologists Opt In?

The Medicare Shared Savings Program (MSSP) had arguably the biggest overhaul in its existence this past December, raising many eyebrows. Although most of us (over 90 percent in 2017) are in “regular” MIPS, the Merit-based Incentive Payment System—see “It’s Year 3. Do You Know Where Your MIPS Is?” on page 18—growing numbers of clinicians are in one of the MSSP tracks. This allows them to be placed in the MIPS-APM category (and depending on which MSSP track even in the advanced APM category, APM standing for alternative payment model).
Radiologists are often part of multispecialty groups that participate in an MSSP ACO. As a result, many radiologists are in these ACOs often without even realizing it. Of the various types of MSSP programs available, most are in the MSSP-1 track, which is upside-only.
“Upside only” means there is no risk of owing money to CMS if the ACO underperforms relative to a benchmark. The modest advantages of being placed in MIPS-APM and the lack of downside risk were some of the reasons networks and physicians opted into MSSP-1.
We should all sign up, then. Right? Well, it’s not so clear now.
With the redesign of the MSSP that was proposed early in 2018 and subsequently finalized toward the end of the year as the “Pathways to Success,” physicians and networks must seriously reconsider enrolling or re-enrolling in the program.
Seema Verma, the CMS administrator, made it clear that her objective was to more aggressively move physicians into risk-based models.
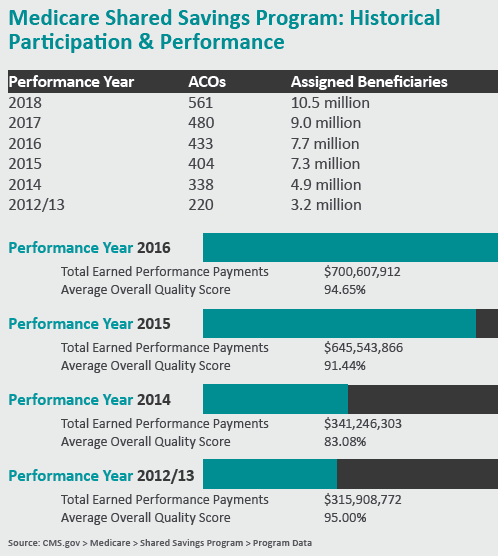
According to CMS, data demonstrated that groups in the risk-based models outperformed those that were upside-only. To that end, CMS confirmed a revamp of the MSSP program that essentially forces all ACOs to progress toward a risk-based model. Tracks 1, 2 and 3 are gone—replaced by the BASIC and ENHANCED tracks, both of which involve risk of some type and which are now five-year contracts (up from three).
Depending on the experience of the organization, those opting into the BASIC track may qualify for up to three years of an upside-only model (A, B and possibly C), but will incur downside risk in at least the last two years (D and E). The ENCHANCED track (essentially equivalent to the former Track 3 model) incurs the highest degree of risk, although it also allows the highest level of possible shared savings.
 What are the implications of these changes?
What are the implications of these changes?
The calculation of shared losses is dependent on the revenue of the participants within an ACO. Because of this, ACOs that include both primary care doctors and specialists should reconsider participation in the MSSP program now that risk is mandated.
Since the loss-sharing limit is calculated as a portion of revenues of ACO participants, it makes sense to exclude as much revenue as possible. As specialists contribute to fewer of the quality metrics in an MSSP compared to primary care doctors, they may be considered less vital in the determination of shared savings compared to their colleagues in primary care. Therefore, excluding specialists in an ACO is an attractive option, as it retains only those participants who most directly impact shared savings, the primary care doctors, yet reduces the exposure to risk by excluding as much revenue as possible for the specialists.
In effect, this further increases the focus on primary care clinicians in generating additional revenue for a group. As an alternative pathway to excluding specialists from their ACO, some multispecialty groups may choose to exit the MSSP altogether.
Another factor that might further push organizations to reconsider participation in MSSP is the concept of low and high revenue ACOs.
The low revenue designation is meant to encourage participation of physician-led ACOs and rural hospitals by allowing for a more gradual transition to risk-based models. However, in so doing, many hospitals will be categorized as a high-revenue ACO and be forced into the highest-risk models much sooner.
Further compounding the issue for organizations is that CMS will make the determination if an organization will be considered low- or high-revenue. This results in some loss of control for organizations over how much risk they are willing to take, since being designated as “high revenue” forces participation in the models with more risk.
The net effect of all these factors may result in increasing numbers of organizations deciding to opt out of MSSP and either returning to or staying in MIPS.
It appears that CMS is betting that a mass exodus out of MSSP is a less likely scenario, since the consequences of an unravelling of the ACO model would have disastrous national consequences given the enormous investment in time, energy and money that has gone into its development and promotion.
Where does this leave the radiologist?
If organizations choose to enter into an MSSP agreement with only primary care doctors, this only further increases the perception of primary care doctors driving quality measures as opposed to specialists such as radiologists. If radiologists are formally excluded from an ACO, we must work even harder to prove to an organization that value in radiology is paramount not only to increasing quality care for our patients but also to potentially decreasing costs. For example, by implementing clinical decision support, an organization could potentially reduce utilization and decrease a network’s costs.
An argument could even be made to the organization that these savings can be shared with the radiology department.
MSSP metrics have always been geared toward primary care measures. The redesign of the program only confirms this framework. It is critical that we radiologists demonstrate to the healthcare community our commitment to quality.
In fact, regardless of whether or not radiologists are part of an organization that is participating in this new brand of MSSP, it remains in our best interest to actively demonstrate quality. Many metrics are available for us to measure the quality of the care we provide our patients. Many of these are available as convenient registries that the ACR offers (DIR, GRID, NMD and R-SCAN, among many others).
Now more than ever in this rapidly changing environment, radiologists must actively demonstrate quality to the healthcare industry and, more importantly, to our patients. The time has never been more right to prove our value.
Dr. Lee is a clinical associate professor at Thomas Jefferson University and section chief of neuroradiology at Philadelphia-based Einstein Healthcare Network.
Clinical Associate Professor, Thomas Jefferson University
Philadelphia
Among the additional posts Ryan Lee, MD, MBA, holds at Einstein are medical director of MRI, chair of the MACRA subcommittee and MRI safety officer. His areas of expertise include radiation management in imaging and radiology clinical decision support, and he several quality and safety committees within the Einstein Healthcare Network.
Dr. Lee is active with the American College of Radiology, serving as chair of its CDS registry steering committee and chair of the quality and safety committee of the ACR’s commission on general, small, emergency and/or rural practice.
He also serves as president of the Philadelphia Roentgen Ray Society and is a member of the noninterpretive skills committee of the American Board of Radiology.